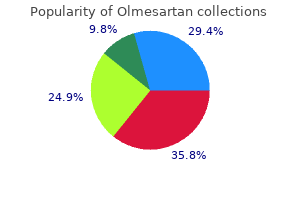
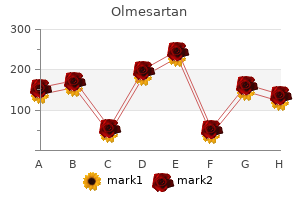
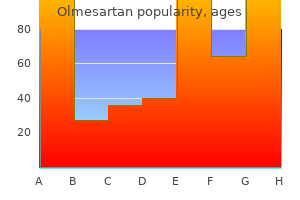
Olmesartan
"Order olmesartan now, blood pressure medication starting with v".
By: S. Finley, MD
Medical Instructor, Lake Erie College of Osteopathic Medicine
This restricts the development of the discipline and requires an element of flexibility to enable the discipline to become embedded in the academic environment heart attack bpm cheap 40mg olmesartan free shipping. This can create great difficulties for departments arrhythmia on ultrasound buy olmesartan 10 mg visa, and there is a danger in these situations that educational standards may be compromised in an effort to maintain the service blood pressure how to take order olmesartan 40 mg fast delivery. Efforts must be made by the educational institutions to maintain standards blood pressure cuff name order 10mg olmesartan mastercard, even in very difficult situations, and to try to work with clinical departments to consider innovative approaches towards graduate retention in the national workforce. This is very applicable in radiotherapy, where a team approach is essential to good practice. In low and middle income resource settings, it is crucial that tasks, roles and responsibilities are shared, and high quality education for all professionals is the key to achieving this [17. The influence of education the factors outlined above must be considered from an educational perspective as greater understanding can lead to improved quality of care and 263 greater efficiency and cost effectiveness. Correct image acquisition during treatment preparation, for instance, can reduce the need for repeat scans. Routine chart checks can detect and/or prevent incidents; clear and detailed set-up instructions can save unnecessary delays at first treatment, and careful management or documentation of acute toxicities, with early referral/intervention, may prevent treatment interruptions and reduce discomfort for the patients in both the acute and late settings. Financial constraints at the departmental level may be reflected in high level technological developments with diminishing resources and a possible changing workforce profile. This could free other professionals to take responsibility for more complex elements of treatment preparation and patient care. Two great educators of the past, Socrates and Galileo, saw education in this context. Socrates described education as drawing out what was already within the student [17. Education is a collaborative enabling process between the lecturer and the student to stimulate a continuously enquiring mind. Effective education in radiotherapy is an equalizer bringing professional freedom and impacting on professional practice, multidisciplinary relationships and ultimately the preparation and delivery of optimum treatment to cancer patients. Irrespective of the external influences, the aspiration must be high quality care for all cancer patients, and the education of all health professionals involved in the preparation and delivery of radiotherapy underpins and supports this aspiration. Practitioners draw from their knowledge and past experiences to solve problems that arise in daily practice. Reflective practice can be encouraged through the use of non-didactic teaching methods and problem solving approaches. In this context, educational institutions should provide or support both undergraduate and postgraduate programmes. The success of health care systems depends on a flexible, innovative and adaptive workforce. All members of the workforce must have these competencies, or risk losing autonomy and influence. As technology changes so too does practice, with the current emphasis much more firmly on team work and partnership. It is questionable whether single discipline education can create the correct environment for interprofessional practice. This approach to interdisciplinary education could also be very practical where resources and staff within the educational institutions are limited and would be most appropriately used for teaching the core competencies common to all health professionals. Education and professional practice Education underpins clinical practice, but should encompass more than the acquisition of clinical skills. Professional practice is defined by the ability to distinguish between good and bad practice and to always accept only best practice. Professional practice underpins best practice and implies at least a minimum level of autonomy and accountability. Education should underpin professional practice and as such education and professional practice are inextricably linked.
Prospective heart attack mayo clinic cheap olmesartan 40 mg without a prescription, observational registry of branded imatinib and nilotinib exposure in pregnant women: voluntary post-authorization safety study blood pressure chart uk pdf cheap 20mg olmesartan free shipping. Prospective pulse pressure of 53 order olmesartan from india, observational registry of branded imatinib and nilotinib exposure in pregnant women: Voluntary post-authorization safety study arrhythmia signs and symptoms 40 mg olmesartan otc. Using proactive awareness activities to recruit patients for a pregnancy exposure registry Description the Ribavirin Pregnancy Registry is a component of the Ribavirin Risk Management Program. It was designed to evaluate the association between ribavirin and birth defects occurring in the offspring of female patients exposed to ribavirin during pregnancy or the 6 months prior to conception, as well as female partners of male patients exposed to ribavirin during the same time period. The registry collects prospective, observational data on pregnancies and outcomes following pregnancy exposure to ribavirin. However, ribavirin showed teratogenic properties in all animal models tested, making pregnancy exposure a concern. Health care professionals have insufficient data on the teratogenic properties of ribavirin in humans to counsel pregnant women exposed to ribavirin either during pregnancy or in the 6 months prior to conception. The registry was established to gather prospective data on ribavirin exposure in pregnancy and pregnancy outcomes to better understand the actual risk. The registry collects data on direct exposures through the pregnant female and indirect exposures through her male sexual partner. The registry collects minimal, targeted data at each trimester and at the outcome of the pregnancy through the obstetric health care providers. For live births, the registry collects data at 6 months and 12 months after the birth by contacting the pediatric health care provider. To gather data on these patients, the registry needed to develop proactive awareness activities to make patients and providers aware of the program and encourage enrollment without promoting ribavirin use during pregnancy. Proposed Solution the registry team developed a multipronged approach to recruiting patients. First, the team developed a comprehensive Web site with information for patients and providers. The Web site contains fact sheets, data forms, information on how to participate, and contact information. Chronic hepatitis C presents a serious health concern for approximately three million Americans, as the infection, if left untreated, can lead to end-stage liver disease, primary liver cancer, and death. Using proactive awareness activities to recruit patients for a pregnancy exposure registry (continued) Proposed Solution (continued) the site also contains a complete slide set that health care providers can use for teaching activities. While the site contains detailed information on the scientific reasons for the registry, the tone and content of the Web site are patient friendly, making it a good resource for both potential patients and providers. Next, the team began targeting professional service groups whose members might treat patients with ribavirin exposure during pregnancy. The groups included hepatologists, gastroenterologists, obstetricians, and pediatricians. As a result of these efforts, the American Gastroenterological Association placed a link for the registry Web site on its Web site, and the American Association for the Study of Liver Diseases posted on its Web site an expert opinion piece written by the former registry advisory board chair. The registry team also raised awareness among professional groups by attending conferences. In 2005, the team presented a poster about the registry, including some information on demographics and program objectives, at the Centers for Disease Control and Prevention National Viral Hepatitis Prevention Conference. In 2009, the team presented a poster at the International Society for Pharmacoepidemiology and in 2010 at the conference of the Teratology Society. In 2010, to expand awareness efforts to health care providers, the registry published results after five years of enrollment, even though the targeted sample size had not been reached. Beginning in 2012, the registry began providing the executive summary of its annual interim report to health care providers upon request; this summary provides the most up-to-date snapshot of registry activity. To raise awareness among patients, the team talked to hepatitis C patient advocacy groups. The registry gained exposure with patients when one patient group wrote an article about the registry for its newsletter and included the registry phone number on its fact sheet. This effort led to many patient-initiated enrollments, despite the lack of patient incentives. In working with patients, the registry has found that emphasizing the goal, which is to gather information to help future patients make better decisions, resonates with patients.
The external review follows as described above under "Resolving conflict of interest" in the preface blood pressure chart discount olmesartan 10 mg with mastercard. It is likely that shared-decision making will plan a major role in arriving at the management decision arrhythmia specialist cheap olmesartan american express. For policy makers-policy making will require substantial debate and involvement of many stakeholders heart attack brain damage purchase 20mg olmesartan amex. Grading the Certainty of Evidence for each Consensus Based Statement High = Further research is very unlikely to change our confidence in the estimate of effect pulse pressure of 10 cheap 20 mg olmesartan free shipping. Moderate = Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low = Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. The recommendation is based largely very low quality studies and/or on expert opinion. Consensus Based Statement without determination of certainty: When there are either no published studies, or very limited and/or very weak evidence, a consensus statement without any category of certainty of evidence was developed. Strong Moderate 29 Conditional Very Low 30 N/A Very Low 31 Conditional Low 32 Conditional Very Low 33 Conditional Moderate 34 Conditional Moderate 35 36 N/A Very Low N/A Very Low 657 21 658 659 660 661 662 663 664 665 666 667 668 669 670 671 672 673 674 675 676 677 678 679 680 681 682 683 684 685 686 687 688 689 690 691 692 693 694 695 696 697 698 699 700 701 Clinical history and physical examination Consensus Based Statement # 1: We recommend that the clinician complete a detailed history and a physical examination in a patient presenting with symptoms of rhinitis. Strength of Recommendation: Strong Certainty of Evidence: Low Consensus Based Statement # 2: We recommend that for patients presenting with rhinitis symptoms, a review of all current medications should be completed to assess if drug-induced rhinitis may be present. The history should include the success or failure of past therapeutic interventions, including self-prescribed over-the-counter medications, homeopathic agents, or physician-prescribed treatments. The overall medical, social, and psychiatric history, medication history (current and past), environmental exposures in the home or workplace, and family views on disease state and healthcare should be included in the patient history. As the final therapeutic decisions will involve shared decision-making, the history should explore the wishes and desires of both the patient and family in selecting diagnostic procedures and therapeutic interventions, including their willingness to adhere to these therapies. The use of validated questionnaires is more beneficial for excluding allergic rhinitis than for confirming allergic rhinitis. The use of one validated 4-question screening tool has been shown to have a high negative predictive value for positive skin prick tests to common aeroallergens (193). Furthermore, if a patient has a late onset of symptoms (> age 45), no family history of allergies, no seasonality of symptoms or symptoms around cats, dogs or other furry pets and has trouble with non-allergic triggers such as deodorants/fragrances, the likelihood of having a component of non-allergic rhinitis before diagnostic skin or serologic testing is 98% predictive (194). While the history has greater reliability and predictive value than solely relying upon the physical exam, the combination of history and physical exam is still advised(195). These co-morbid conditions may include accompanying allergic conjunctivitis, otitis, eustachian tube dysfunction, chronic rhinosinusitis with and without nasal polyps, asthma, and/or atopic dermatitis (1) (196-198). Furthermore, a patient with a history of rhinitis who is asymptomatic or minimally symptomatic at the time of the physical exam, may have minimal or no abnormal findings. The nasal pharyngeal exam can usually be accomplished with the use of a nasal speculum with appropriate lighting or an otoscope with a nasal adapter(1), although these provide a more limited view of the nasal cavity than a nasopharyngolaryngoscope. For mucosal edema that prohibits an adequate exam, the use of a topic nasal decongestant may reduce turbinate mucosal edema, allowing for better visibility and delineation of abnormal findings. A pneumatic otoscope allows for the assessment of tympanic membrane mobility and presence of transudative fluid. At times, an impedance tympanometer may also be of benefit to assess tympanic membrane mobility and the presence/absence of middle ear fluid. A nasopharyngolaryngoscope exam should be completed when a more extensive nasal/pharyngeal/laryngeal exam is required due to suspected structural or functional abnormalities, inadequate therapeutic response or a 24 740 741 742 743 744 suspected complication. Physical examination of patient presenting with symptoms compatible with rhinitis (modified from Table V in 2008 Rhinitis Practice Parameter) (1) 745 746 747 748 749 750 751 752 753 754 755 756 757 758 759 760 761 762 Note: this list is not intended to be totally inclusive. Elements of the examination that will assist in the differential diagnosis of rhinitis or that may indicate complications of treatment are included. General observations: facial pallor, elongated facies, preferred mouth breathing, and any evidence of systemic disease. Eyes: Excessive lacrimation, erythema and swelling of the bulbar and/or palpebral conjunctiva, cobblestoning of the tarsal conjunctiva, swelling or dermatitis of outer eyelids, Dennie-Morgan lines, or venous stasis below the lower eyelids (``allergic shiners' which may occur in allergic or non-allergic rhinitis). Nose: Reduced patency of nasal valve; alar collapse; transverse external crease; external deformity such as saddle nose (loss of nasal bridge that may occur from nasal trauma or systemic disorders such as relapsing polychondritis, granulomatosis with polyangiitis, cocaine abuse, or some systemic infections); septal deviation or perforation, spurs, ulcers, perforation, prominent vessels, or excoriation; nasal turbinate hypertrophy, edema, pallor or erythema, and crusting; discharge (amount, color, consistency), and nasal polyps. Ears: Tympanic membrane dullness, erythema, retraction, perforation, reduced or increased mobility, and air-fluid levels. Oropharynx: Halitosis, dental malocclusion or high arched palate associated with chronic mouth breathing, tonsillar or adenoidal hypertrophy, cobblestoning of the oropharyngeal wall, pharyngeal postnasal discharge, temporomandibular joint pain or clicking with occlusion, furrowing, coating, or ulceration of tongue or buccal mucosa. Neck: Lymphadenopathy, or tenderness, thyroid enlargement or nodule Chest: Signs of asthma such as wheezing, or other abnormal or diminished sounds by auscultation.
Syndromes
- Congestive heart failure
- Excessive bleeding
- Polythiazide (Renese)
- Low-fat dairy products
- CBC
- Provide walking assistance for safety reasons, especially on uneven ground.
- Tolazamide (Tolinase)
- Return of the varicose vein over time
- You are obese
- Electrolyte changes (abnormal levels of sodium and potassium in the blood)
Education on how to turn in bed blood pressure chart low purchase olmesartan 20 mg amex, compress the chest when coughing and the irritation of the trachea with suctioning are important points blood pressure medication by class discount olmesartan 20mg online. Women should be instructed in the use of a post surgical bra to minimize tension on the sternotomy wound and sutures heart attack in sleep cheap olmesartan 40 mg on-line. Myasthenia gravis does not interfere with gas exchange itself heart attack in women olmesartan 40mg mastercard, but the capacity of the chest muscles to support respiration. This condition can happen quickly with little or no warning and requires immediate emergency medical care. Observe the patient for signs of shortness of breath or increased respiratory effort. This is especially important for patients on long term corticosteroids (prednisone) who are at risk for bone loss. If on steroids excess calories and carbohydrates can increase risk for diabetes and weight gain. This is especially important due to fluid retention secondary to steroid medication. The timing of immunizations is important especially if patients are immunosuppressed and should be discussed with the treating physicians. Atypical reactions associated with use of angiotensin-converting enzyme inhibitors and apheresis. Fenichel, J Jankovic, ButterworthHeinemann Publishers, 5th edition, Chapter 82 pp. It almost goes without saying that a myasthenic patient should be under the care of a neurologist who specializes in treating these individuals. Patients with no symptoms or ocular symptoms only will tend to fare better than those with limb weakness or bulbar symptoms (dysarthria, dysphagia, etc. Patients with more severe symptomatology should be referred to their treating neurologist for adjustments or additional treatment before elective surgery. For more urgent cases, more severe symptoms may point to a need for continued postoperative ventilation. The anesthesiologist will want to know how long the patient has been diagnosed with myasthenia gravis, what the presenting symptoms were and how this compares to current symptoms. Every patient with this condition should be asked if he or she has trouble laying flat. Stridor or subjective shortness of breath in the supine position may indicate thymic hyperplasia severe enough to compress the trachea. These patients present a challenge because the induction of general anesthesia (with cessation of respiratory drive and relaxation of the tracheobronchial tree) may lead to airway compression severe enough to prevent ventilation of the patient even with an endotracheal tube in place, a potentially deadly situation. Such paAnesthesia Issues tients require airway management (intubation) with maintenance of spontaneous respiration, perhaps even awake. Many patients with cholinergic excess will have symptoms severe enough to present to an emergency department and will have been managed appropriately before elective surgery. Cholinesterase inhibitors which act by blocking the degradation of acetylcholine include pyridostigmine. Arrangements should be made so this medication can be administered prior to anesthesia induction and at appropriate time intervals after recovery from anesthesia. Intramuscular administration of the drug should be use if a parenteral route is necessary. Intrave- 86 nous injections may exert their effects too quickly and may precipitate cholinergic excess. Patients who have been on chronic steroid therapy may need supplemental steroid doses to deal with the stresses of moderate to major surgery, though this is a source of controversy. Its most important side effect is nephrotoxicity that may pose some difficulty for the anesthesiologist. Azathioprine, a purine analog, and methotrexate, a folic acid analogues, target immune cell replication. They may lead to bone marrow suppression, liver toxicity, nephrotoxicity and other less serious effects (Marczin N, 2004). With the patient supine, one should listen over the trachea with a stethoscope for stridor and check for tracheal deAnesthesia Issues viation. A chemistry panel (including blood glucose) is usually warranted for moderate to major surgery. Abnormalities in electrolyte concentrations can interfere with neural conduction and exacerbate muscle weakness.
Purchase olmesartan 20mg with amex. Garlic The Ultimate Remedy Medical Course.
