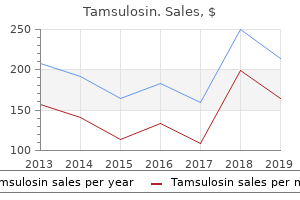
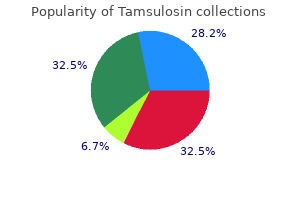
Tamsulosin
"Buy 0.4 mg tamsulosin fast delivery, prostate yourself".
By: V. Gorok, M.B.A., M.B.B.S., M.H.S.
Co-Director, University of Oklahoma School of Community Medicine
In some cases prostate cancer cure purchase tamsulosin no prescription, the psychosis may have a distinct manic flair: one patient (Besson 1980) was `grandiose prostate cancer facts purchase tamsulosin with a visa. The personality change may be non-specific; however androgen hormone joint cheap tamsulosin 0.2 mg, a frontal lobe syndrome may be prominent (Austin et al mens health lunch ideas tamsulosin 0.4 mg online. As might be suspected, in addition to cognitive deficits, the dementia seen in metachromatic leukodystrophy is also often marked by delusions, hallucinations, and frontal lobe symptomatology (Alves et al. Nerve conduction velocity studies may reveal slowing in patients who lack clinical evidence of a peripheral neuropthy; however, it must be kept in mind that such studies may be normal. An often mentioned, but rarely seen, finding in metachromatic leukodystrophy is non-filling of the gallbladder on cholecystography, which occurs secondary to infiltration of the gallbladder by sulfatides. Assays of leukocytes reveal decreased aryl sulfatase A activity, and assays of peripheral nerve tissue (obtained at sural nerve biopsy) or of urinary sediment will reveal increased sulfatide content. The phenomenon of metachromasia, from which this disorder derives its name, may also be observed in peripheral nervous tissue or urinary sediment. Both cresyl violet and toluidine blue undergo a chromatic metamorphosis, turning from violet or blue to brown or golden-brown, respectively, when applied to affected cells in the peripheral nerve or urinary sediment. Of interest, the increased sulfatide content in peripheral nervous tissue and renal epithelial cells accounts for the metachromasia. Sulfatides are positively charged, and their excessive presence reorients the negatively charged molecules of cresyl violet or toluidine blue, thereby changing their color. Within the central nervous system, widespread demyelinzation is seen, and this is especially evident in the centrum semiovale. In severe cases, the white matter of the centrum semiovale may be shrunken down to a thin gliotic remnant, with only relative sparing of the U-fibers, such that there is very little intervening tissue between the depths of the sulci and the lateral ventricles. The cerebellar white matter is affected in a similar fashion, and there is also peripheral demyelinization. Rarely, rather than occurring secondary to a mutation in the gene for arylsulfatase A, metachromatic leukodystrophy may occur secondary to a mutation in a gene on chromosome 10 coding for a sulfatide activator protein (Schlote et al. This protein acts as an essential cofactor for arylsulfatase A and, in its absence, all of the biochemical defects seen with mutations in the gene for arylsulfatase A also accrue. Differential diagnosis Differential diagnostic considerations vary according to the age of the patient. Juvenile-onset cases may be confused with adrenoleukodystrophy; however, in adrenoleukodystrophy one also sees either a hemianopia or cortical blindness, findings not seen in metachromatic leukodystrophy. Adult-onset cases may, depending on their presentation, raise several differential considerations. Presentations with psychosis may be indistinguishable from schizophrenia until other signs and symptoms, such as ataxia or peripheral neuropathy, emerge, or until a dementia supervenes. Presentations with a personality change of the frontal lobe type or with a dementia may raise the possibility of frontotemporal dementia, and the differential here may also rest on the emergence of a peripheral neuropathy or ataxia. As noted earlier, diagnosis rests on demonstrating decreased aryl sulfatase A activity in leukocytes and in finding increased sulfatide content in peripheral tissues, and it must be stressed that both tests must be positive. Course the disease is gradually progressive, with death within 20 years in the late infantile or juvenile forms; in the adult form, death may be delayed for up to 15 years. Etiology As noted, metachromatic leukodystrophy is a recessively inherited disorder, and occurs secondary to any of a large number of mutations in the gene for arylsulfatase A, found on chromosome 22 (Barth et al. Thus, onset may be in childhood (at an average age of 8 years), adolescence, or adult years, and the primary site may be cerebral, spinal, or adrenal. Childhood-onset adrenoleukodystrophy usually presents with cerebral symptomatology, often with a personality change and visual symptoms. These patients may become withdrawn and irritable, and school performance declines. Varying degrees of hemianopia or cortical blindness may occur, followed by a dementia accompanied by spasticity (Moser et al. Adolescent-onset adrenoleukodystrophy tends to present in a fashion similar to that of the childhood-onset form. Adult-onset adrenoleukodystrophy tends to present with spinal cord involvement, adrenal failure or, less commonly, with cerebral involvement; in cases that present with cord involvement or adrenal failure, long-term follow-up reveals the development of cerebral involvement in a significant minority (van Geel et al. Cerebral involvement produces a dementia that may be nonspecific in character, or which may be marked by manic symptoms (Weller et al. Peripheral nerve involvement tends to be mild and may in some cases only be apparent with nerve conduction velocity studies. Seizures occur in about one-fifth of all patients, usually late in the course of the disease.
Diagnosis: Mucinous cystadenoma of the ovary the answer is E: Mucosa of the endocervix mens health how to last longer in bed order tamsulosin 0.4mg without a prescription. This meso- 48 A 25-year-old woman presents with a 6-month history of breast enlargement and menstrual irregularities prostate oncology questions discount 0.2mg tamsulosin fast delivery. An endometrial biopsy 3 months previously showed complex hyperplasia without atypia prostate cancer gleason score cheap tamsulosin 0.2mg mastercard. Following removal of this neoplasm prostate cancer metastasized generic 0.4 mg tamsulosin amex, a marked decrease in serum levels of which of the following hormones would be expected in this patient Evacuation of the uterus by suction curettage reveals grapelike clusters and fetal parts. Cytogenetic examination of this tissue will most likely demonstrate which of the following genetic patterns Compared with multiparous women, this patient is at increased risk of developing a neoplasm in which of the following anatomic locations Common epithelial tumors of the ovary, in order of decreasing frequency, include: serous tumors that resemble the epithelium of the fallopian tube (choice B); mucinous tumors that mimic the mucosa of the endocervix (choice E); endometrioid tumors that are similar to glands of the endometrium (choice C); clear cell tumors that display glycogen-rich cells that resemble endometrial glands in pregnancy (choice A); and transitional cell tumors that resemble the mucosa of the bladder (choice D). These tumors are broadly classified as benign, borderline (atypical proliferative), and malignant. Diagnosis: Mucinous cystadenoma of the ovary 6 the answer is D: Tubo-ovarian abscess. The infection is a frequent cause of acute salpingitis and pelvic inflammatory disease. The organisms ascend through the cervix and the endometrial cavity, where they cause an acute endometritis. The bacteria then attach to mucosal cells in the fallopian tube and elicit an acute inflammatory reaction, which is confined to the mucosal surface (acute salpingitis). From the tubal lumen, the infection spreads to involve the ovary, sometimes resulting in a tubo-ovarian abscess. The healing process distorts and destroys the plicae of the fallopian tube, often leading to sterility. Diagnosis: Gonorrhea, pelvic inflammatory disease the answer is A: Extramammary Paget disease. Paget disease of the vulva is named after similar-appearing tumors in the nipple and extramammary sites, such as the axilla and perianal region. The typical Paget cell has a pale, vacuolated cytoplasm that contains glycosaminoglycans. Women with Paget disease of the vulva complain of pruritus or a burning sensation for many years. Lichen sclerosis is an inflammatory disease of the vulva, which is often associated with autoimmune disorders such as vitiligo, pernicious anemia, and thyroiditis. The condition is represented by white plaques, atrophic skin, a parchment-like or crinkled appearance, and, occasionally, marked contracture of the vulvar tissues. Histologically, there is hyperkeratosis, loss of rete ridges, and a homogeneous, acellular zone in the upper dermis. Women with symptomatic lichen sclerosis have a 15% chance of developing squamous cell carcinoma. Condyloma acuminatum is a benign, exophytic, papillomatous lesion on the skin or mucous membranes of the lower female genital tract. Types 16, 18, 31, and 45 are the most representative high-risk types linked to intraepithelial neoplasia and invasive cancer. The other pathogens do not infect the cervix and do not produce this histopathologic appearance. Lymphogranuloma venereum is a sexually transmitted infection that is endemic in tropical countries but rare in developed ones. This organism has been found in the genital tract of about 8% of asymptomatic women and in 20% of women presenting with symptoms of a lower genital tract infection.
Buy online tamsulosin. Why Aloe Vera is Good for Men - Make Juice with Aloe Vera Gel Lemon and Honey at Home.
In such cases man health yahoo generic 0.2mg tamsulosin, a lacune is typically found in the ventrolateral thalamus: occasionally prostate cancer fund generic 0.2mg tamsulosin with visa, when the lacune is surrounded by a substantial amount of edema prostate cancer xray generic 0.2 mg tamsulosin with amex, involvement of the adjacent posterior limb of the internal capsule may cause a contralateral hemiplegia prostate cancer lung metastasis discount 0.2mg tamsulosin with mastercard, which, however, is usually relatively mild and clears as the edema resolves. In the months following a pure sensory stroke, a minority of patients may begin to experience chronic painful dysesthesiae in the involved limbs. Lacunes affecting the anterior or central portions of the thalamus (Bogousslavsky et al. Over time, patients typically become alert but are left with memory deficits (reflecting involvement of the mammillothalamic tract) or a frontal lobe syndrome (with involvement of the dorsomedial nucleus); furthermore, when the lacune is on the left, aphasia may occur and, when on the right, neglect may be seen. Early on there may also be a dysarthria or mild hemiparesis, both transient, and agitation or restlessness, especially when the lacune is in the right caudate nucleus. Here, all, or almost all, of the lenticulostriate arteries on one side are occluded, resulting in a relatively large infarction involving the posterior limb of the internal capsule and the putamen. Symptomatically, as might be expected, such a giant lacune generally presents with a contralateral hemiplegia that may be accompanied, if the lesion is on the left, by a transcortical motor aphasia or, if the lesion is on the right, by left neglect. In such a scenario, the lack of collateral supply to the area nourished by the lenticulostriate arteries leads to infarction, whereas the cerebral cortex, being supplied with rich collaterals, may escape infarction. Clinically, patients may experience any of the symptoms of ischemic infarction just described, with one critical difference: after a brief period of time, the symptoms resolve completely, with a full restoration of prior functional ability. Thus, it is probably best to reserve this diagnosis for cases where symptoms last no longer than a half hour, and in no case for more than an p 07. The transient reduction in blood flow may be due to either an embolus that fragments and passes on in a few minutes, or to temporary low flow past a thrombus or through a stenosed artery, as may occur during an episode of systemic hypotension. Given this, it is appropriate, if one is not already done, to immediately institute a work up, as described below, just as if the patient had already had an ischemic infarction, and then to pursue appropriate treatment. Such ventricular extension is most common when the hemorrhage is close to a ventricle, as may be seen with a caudate hemorrhage secondary to rupture of the recurrent artery of Heubner or a thalamic hemorrhage secondary to rupture of the thalamoperforating artery; putaminal hemorrhages, secondary to rupture of a lenticulostriate artery, may also extend into the nearby lateral ventricle. In cases of cerebellar hemorrhage, the proximity of the hemorrhage to the brainstem sets the stage for another mechanism of catastrophic worsening, namely compression of the underlying brainstem. When this occurs, coma and death may occur, and surgical decompression is mandatory. In a significant minority seizures may also occur during the initial presentation (Caplan 1988). Most cases of subarachnoid hemorrhage present in a catastrophic fashion (Suarez et al. The headache may rise to its maximal intensity over seconds, and is often described by patients as the worst in their lives. In some cases when the arterial eruption is directed toward the parenchyma, a jet of blood may pierce into the brain, causing an intracerebral hemorrhage. Seizures may complicate the clinical picture within the first 24 hours, and are seen in up to one-fifth of all patients. Patients who survive the initial event are at risk for significant complications (Hijdra 1988) over the following weeks, including rebleeding, vasospasm with cerebral infarction, and the development of hydrocephalus. Rebleeding may occur in up to 20 percent of patients and, although it is most common within the first 24 hours, the risk extends for two or more weeks. Vasospasm of cerebral arteries passing through the subarachnoid blood may occur, leading to clinically evident ischemic infarction in approximately one-third of all patients (Hijdra et al. The risk for vasospasm appears within the first few days, peaks at 50 days and then subsides by 2 weeks. Acute hydrocephalus, with headache and lethargy, may be seen in up to 20 percent of patients within the first hours or days, and occurs secondary to blockage, by clotted blood, of the exit foramina of the fourth ventricle. Dementia With multiple ischemic infarctions or intracerebral hemorrhages, patients may be left demented. This may occur with either cortical or white matter infarcts, producing a multi-infarct dementia (discussed further in Section 10. Subarachnoid hemorrhage may also be followed by a dementia, due either to chronic hydrocephalus or multiple infarctions due to vasospasm. Cerebral venous thrombosis, if accompanied by multiple venous infarctions, may also leave patients demented; in the absence of these, most patients, if they survive, do so without cognitive sequelae. Post-stroke depression In the weeks or months following stroke, close to one-half of all patients will develop a depression of variable severity. The location of the infarct or hemorrhage plays a part here, with lesions in the anterior portions of the frontal lobes being more likely to cause depression.
In addition to these linguistic problems androgen hormone receptor buy generic tamsulosin line, these children often have other difficulties mens health 9 best teas buy 0.2 mg tamsulosin mastercard, including anxiety mens health 55 style rules purchase 0.2mg tamsulosin with mastercard, emotional lability prostate cancer 6 out of 10 buy tamsulosin 0.4 mg on-line, and, especially in boys, aggressiveness and hyperactivity. Course Although some degree of improvement may gradually occur during adolescence, for the most part this is a chronic disorder. Etiology Developmental dysphasia is familial and linkage has been found to loci on chromosomes 13, 16, and 19 (Bartlett et al. Magnetic resonance imaging has demonstrated both a reversed asymmetry of linguistic cortex (De Fosse et al. Electroencephalogram studies have revealed an increased incidence of interictal epileptiform discharges (Nasr et al. One autopsy study demonstrated a dysplastic gyrus on the inferior surface of the left frontal cortex (Cohen et al. Overall, it appears probable that developmental dysphasia occurs secondary to a genetically mediated disruption of normal neuronal migration to the peri-sylvian cortex, resulting in gyriform or dysplastic abnormalities. It is not clear whether the interictal epileptiform discharges are merely epiphenomenal, reflecting an unexpressed epileptogenic potential of dysplastic cortex, or are perhaps indicative of an epileptic process that, at least theoretically, could disturb normal development or function of the linguistic cortex. Both autism and childhood-onset schizophrenia may be characterized by linguistic disturbances similar to those seen in the mixed form of developmental dysphasia; however, in these disorders other symptoms also occur. Acquired dysphasia may be seen with head trauma, encephalitis, tumors, and the Landauleffner syndrome, and has also been reported as a side-effect of topiramate (Gross-Tsur and Shalev 2004). At present, there is no method whereby these children can be confidently distinguished from those whose development will eventually plateau at a lower than normal level, and consequently long-term clinical follow-up is required. Some practitioners recommend treatment with anti-epileptic drugs in cases with interictal epileptiform discharges; however, this is controversial and there are no controlled studies to support this practice. First described by Hinshelwood in 1896, this is a common disorder, seen in up to 4 percent of school age children. Although once thought to be far more common in boys, recent epidemiologic work suggests that the prevalence is roughly equal in boys and girls. Synonyms include reading disorder, specific reading disability, and congenital word blindness (Orton 1925). Differential diagnosis Deafness may simulate developmental dysphasia, and all children in whom this diagnosis is considered should have audiometry. Severe deprivation may stunt language development; however, these children, in contrast to those with dysphasia, typically show rapid gains when placed in a linguistically stimulating environment. Clinical features Depending on its severity, developmental dyslexia may first come to light anywhere between the ages of 6 and 9 years as the child falls behind his or her peers in the acquisition of reading skills. In attempting to read out loud, these young patients seem to stumble over certain words: they may skip words and go on to the next, or they may misread a word and say one that p 09. Reading comprehension is impaired and, after finally, and haltingly, reading a paragraph, the child may be unable to paraphrase it in his or her own words. In striking contrast, if the same paragraph is read out loud to the child, he or she may then be able to paraphrase it with little difficulty. In some cases entire sentences may be reversed, with the written words reading from right to left on the page. Mental retardation is characterized by deficient reading, but here, in contrast to developmental dyslexia, one finds deficits in other academic skills. This is probably an uncommon disorder, and is probably more common in boys than girls. Course Although there may be some spontaneous improvement over long periods of time, the overall natural course is marked by a chronic difficulty in reading. Penmanship may or may not be poor; at times the penmanship far outshines what is actually written. Importantly, and in stark contrast to what they write, these children are often able to express themselves quite well when speaking. Etiology Developmental dyslexia is clearly familial; concordance among dizygotic twins is about 25 percent, and among monozygotic twins it rises to about 50 percent. Autopsy studies in males reveal cortical dysgenesis, which, although widespread, is concentrated in the left peri-sylvian areas (Galaburda et al.
