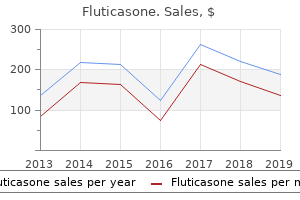
Fluticasone
"Order fluticasone 500 mcg overnight delivery, asthma symptoms 3 year old".
By: R. Dawson, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Associate Professor, University of South Florida College of Medicine
In most instances central venous access will be required for the intravenous administration of cytotoxics to children; care is required to avoid the risk of extravasation (see Side-effects of Cytotoxic Drugs and their Management) asthma treatment no medication purchase fluticasone pills in toronto. Contraceptive advice should be given to men and women before cytotoxic therapy begins (and should cover the duration of contraception required after therapy has ended) asthma definition 8 bells cheap fluticasone 500 mcg amex. Alkylating drugs can have an adverse effect on gametogenesis asthma definition 7-day 500mcg fluticasone with amex, which may be reversible particularly in females asthma treatment plan generic fluticasone 250mcg amex. Cytotoxic drugs for the treatment of cancer should be given as part of a wider pathway of care that is coordinated by a multi-disciplinary team. Injectable cytotoxic drugs should only be dispensed if they are prepared for administration. Oral mucositis Good oral hygiene keeps the mouth clean and moist and helps to prevent mucositis; prevention is more effective than treatment of the complication. For children under 6 months or when it is not possible to brush teeth, carers should be instructed how to clean the mouth using an oral sponge moistened with water or with an antimicrobial solution such as diluted chlorhexidine. Nausea and vomiting Nausea and vomiting cause considerable distress to many children who receive chemotherapy, and to a lesser extent abdominal radiotherapy, and may lead to refusal of further treatment; prophylaxis of nausea and vomiting is therefore extremely important. Symptoms may be acute (occurring within 24 hours of treatment), delayed (first occurring more than 24 hours after treatment), or anticipatory (occurring prior to subsequent doses). Delayed and anticipatory symptoms are more difficult to control than acute symptoms and require different management. Due to the risks of neurological sideeffects, metoclopramide hydrochloride should only be used in children as a second-line option. Manifestations of such toxicity may not appear for several months or even years after cancer treatment. Careful follow-up of survivors of childhood cancer is therefore vital; national and local guidelines have been developed to facilitate this. Tumour lysis syndrome Tumour lysis syndrome occurs secondary to spontaneous or treatment related rapid destruction of malignant cells. Features, include hyperkalaemia, hyperuricaemia, and hyperphosphataemia with hypocalcaemia; renal damage and arrhythmias can follow. Early recognition of patients at risk, and initiation of prophylaxis or therapy for tumour lysis syndrome, is essential. It should be started 24 hours before treatment; patients should be adequately hydrated (consideration should be given to omitting phosphate and potassium from hydration fluids). It rapidly reduces plasma-uric acid concentration and may be of particular value in preventing complications following treatment of leukaemias or bulky lymphomas. The disodium salts of folinic acid and levofolinic acid are also used for rescue therapy following methotrexate administration. Urothelial toxicity Haemorrhagic cystitis is a common manifestation of urothelial toxicity which occurs with the oxazaphosphorines, cyclophosphamide p. This commonly occurs 7 to 10 days after administration, but is delayed for certain drugs, such as melphalan p. The duration and severity of neutropenia can be reduced by the use of granulocyte-colony stimulating factors; their use should be reserved for children who have previously experienced severe neutropenia. Infection in a child with neutropenia requires immediate broad-spectrum antibacterial treatment that covers all likely pathogens. Appropriate bacteriological investigations should be conducted as soon as possible. Children taking cytotoxic drugs who have signs or symptoms of infection (or their carers) should be advised to seek prompt medical attention. All children should be investigated and treated under the supervision of an appropriate oncology or haematology specialist. If an immunocompromised child has come into close contact with an infectious individual with measles, normal immunoglobulin p.
He found that after a transection between the medulla and the spinal cord asthma yellow zone purchase on line fluticasone, a preparation that he called the encephale isole asthma definition medscape order fluticasone master card, or isolated brain asthma breathing treatment purchase genuine fluticasone line, animals showed a desynchronized (low voltage asthma united states cheap fluticasone online american express, fast, i. Bremer concluded that the forebrain fell asleep due to the lack of somatosensory and auditory sensory inputs. Later studies showed that electrical stimulation of the midbrain reticular core could excite forebrain desynchronization. The waves of postsynaptic potentials in the cerebral cortex are now understood to be due to the intrinsic burst firing of neurons in the thalamus, basal forebrain, and the cortex itself, which produce waves of postsynaptic potentials in cortical neurons. When the membrane potential of burst neurons is close to their firing threshold, they fire single action potentials that transmit sensory and other information. However, when burst neurons have been hyperpolarized to membrane potentials far below their usual threshold for firing sodium action potentials, a low-threshold calcium channel is deinactivated. When the low-threshold calcium channel is triggered, calcium entry brings the membrane potential to a plateau that is above the threshold for firing sodium action potentials. As a result, a series of sodium spikes are fired, until sufficient calcium has entered the cell to activate a calcium-activated potassium current. This potassium current then brings the cell back to a hyperpolarized state, terminating the burst of action potentials. This brings the cell above the threshold for firing sodium action potentials, which are fired in a burst, until this is terminated by a calcium-activated potassium current that hyperpolarizes and silences the cell. Thalamic axons on their way to the cerebral cortex, and cortical projections to the thalamus, give off collaterals to the reticular nucleus as they pass through it. Basal forebrain neurons also fire in bursts that are time-locked to cortical rhythms. Periods of forebrain arousal returned after several days if the animals were kept alive. However, it is clear that the slab of tissue from the rostral pons through the caudal midbrain (the mesopontine tegmentum) contains neural structures that are critically important to forebrain arousal, at least in the acute setting. At the time, little was known about the origins of ascending projections from the mesopontine tegmentum to the forebrain, and the arousal effect was attributed to neurons in the reticular formation. However, more recent studies have shown that projections from the mesopontine tegmentum to the forebrain arise from several well-defined populations of neurons. The major source of mesopontine afferents that span the entire thalamus is a collection of cholinergic neurons that form two large clusters, the pedunculopontine and laterodorsal tegmen- tal nuclei. Other neurons in the cholinergic pedunculopontine and laterodorsal tegmental nuclei send axons into the lateral hypothalamus, where they may contact populations of neurons with diffuse cortical projections (see below). Some of them innervate the midline and intralaminar nuclei of the thalamus, and others pass through the lateral hypothalamus to the basal forebrain and prefrontal cortex. In an awake and aroused individual, this alteration in firing may result in an improvement in signal-to-noise ratio, which may be critical in sharpening cortical information processing to avoid misperception of stimuli, such as occurs during a delirious state. During these periods, eye movements are few and muscle tone drops to very low levels. This usually takes about 45 to 60 minutes, and then the subject often will gradually emerge from the first bout of slow-wave sleep to stage I again. This pattern, which is typical of young adults, changes dramatically across a lifetime. Thus, phenomena such as night terrors, bed wetting, and sleep walking tend to occur mainly during slow-wave sleep in children but disappear as the children become older and spend less time in those sleep stages. These drugs are thought to act directly on the arousal system, inhibiting the firing of its neurons. Populations of neurons in the pre-locus coeruleus area and medial parabrachial nucleus have intense inputs to the basal forebrain. Cell-specific lesions of these neurons produce profound coma, suggesting that they may be a major source of the ascending arousal influence. In addition, along the course of the ascending cholinergic and monoaminergic axons through the rostral midbrain reticular formation, there are many additional neurons that project to the thalamic relay, midline, and intralaminar nuclei. On the other hand, they do not appear to be capable of maintaining a waking state in the case of acute loss of the influence from the mesopontine neurons. Along the course of the ascending arousal systems, as they pass through the hypothalamus, are several hypothalamic cell groups that augment the ascending projection to the basal forebrain and cerebral cortex. These include histaminergic neurons in the tuberomammillary nucleus as well as several populations of neurons in the lateral hypothalamic area, all of which project diffusely to the cerebral cortex and innervate the intralaminar and midline thalamus. Histamine H1 blockers impair wakefulness in both animals and humans,55 and transgenic mice lacking H1 receptors have impairment of arousal responses induced by intraventricular injection of the peptide orexin.
Safe 250mcg fluticasone. Severe Asthma Sufferer Carey Poindexter Is Fighting for Air.
Technical asthma symptoms heartburn buy generic fluticasone 500 mcg line, Legal asthma treatment long-term order fluticasone 500 mcg, and Analytic Considerations for Combining Registry Data With Other Data Sources Case Example 32 asthma 4x4 buy generic fluticasone 500mcg line. By eliminating the need for manual chart abstraction and data entry asthma definition race discount generic fluticasone canada, some barriers to practice participation are removed. A software solution that executes this extraction automatically may take time to set up initially, but minimizes workflow disruption during continued registry participation. Creating a registry interface to incorporate data from multiple electronic health records (continued) Proposed Solution (continued) transfers occur on a schedule determined by each site-some send their data in real time while others send on a monthly basis. Once the registry receives data files, registry staff members review each portion of the data (demographics, vaccinations, office visits, etc. Extensive error checking and validation are completed during the initial specification phase to minimize the amount of manual data checking needed during each transfer. The validation phase involves both technical staff and quality improvement staff at the practices to ensure that the data are transferred and mapped correctly into the registry database. The organization and management of this initiative have required strong internal support from the registry and from participating practices. However, the association quickly realized that it needed to integrate and exchange health information from multiple sources, such as payer claims, pharmacy claims, practice management systems, laboratory databases, and other registry systems, on behalf of more than 150 primary care practices. Technical and security issues in creating a health information exchange Description the Oakland Southfield Physicians Quality Registry is a practice-based registry designed to promote health outcomes and office efficiencies, and to identify early interventions and best practices in primary care practices. Oakland Southfield Physicians 2006 Ongoing 150 Sponsor Year Started Year Ended No. Technical, Legal, and Analytic Considerations for Combining Registry Data With Other Data Sources Case Example 34. Data transfers occur at established intervals, based on record updates or availability of information. A key aspect of the system is the master patient and physician index, which allows data from various sources to be linked to the proper patient. Prior to import, data received in the registry are validated against a master patient and physician index for accuracy. Results Through data sharing with the Oakland Southfield Physicians registry, the practice association has been able to facilitate the alignment of multiple data sources, with evidence-based care guidelines available at point of care-a value partnership striving to improve health outcomes as well as the efficient access to key health care data points. This solution relies on building trust between trading partners in support of both the secure transfer of information and recommended use. The data warehouse also generates monthly "gaps-in-care reports" for physician clinical quality review and patient outreach. When integrating data from many sources, a master patient and physician index can be a critically important tool for ensuring that the incoming data are linked to the appropriate patient. The system must be scalable, must incorporate data from many sources, and must be flexible enough to adapt to the needs of many diverse groups. However, the availability of large amounts of data in electronic formats presents the opportunity to rethink the spontaneous adverse event reporting system. Technical, Legal, and Analytic Considerations for Combining Registry Data With Other Data Sources Case Example 35. Following implementation, more than 200 events were reported over a period of 3 months. Moving to a truly digital system may require a change in the data collected to better align with the way data are collected in electronic formats. While the assessment noted the potential value of such an automated reporting system, it also provided suggestions for improving the quality and utility of the data. Quality assessment of spontaneous triggered adverse event reports received by the Food and Drug Administration. Secondary use of electronic health record data: spontaneous triggered adverse drug event reporting. Interfacing Registries With Electronic Health Records References for Chapter 15 1. Development of an electronic health record-based Clinical Trial Alert system to enhance recruitment at the point of care. The Common Data Element Dictionary-A Standard Nomenclature for the Reporting of Phase 3 Cancer Clinical Trial Data. Technical, Legal, and Analytic Considerations for Combining Registry Data With Other Data Sources 20. Distributed health data networks: a practical and preferred approach to multi-institutional evaluations of comparative effectiveness, safety, and quality of care.
This technique should only be used by experienced clinicians due to the risk of cross-contamination secondary to inadvertent transducer or needle movement asthma symptoms from acid reflux generic fluticasone 250mcg free shipping. The choice of aseptic technique used during the ultrasound-guided procedure should be documented in the report asthma humidifier 250mcg fluticasone overnight delivery. Local anesthesia should be administered in accordance with procedural requirements and practicespecific standards asthma definition resolution order generic fluticasone from india. The needle should be advanced through the skin and guided to the target along the appropriate trajectory using one of the following techniques: a asthma handouts purchase fluticasone cheap. Thus, the long axis of the transducer is parallel to the long axis of the needle, producing an in-plane sonographic view of the needle. Correlative view from the side demonstrating the colinearity of the transducer and the needle. The entire shaft (yellow arrows) and tip (green arrow) can be visualized using the in-plane approach, facilitating optimal control for ultrasound-guided procedures. The in-plane technique can be performed freehand or with the assistance of a needle guide. The in-plane technique is often preferred during ultrasound-guided procedures because the needle tip and shaft are visualized throughout the entire procedure. During the in-plane approach, the conspicuity of the needle is primarily dependent on the angle of the needle with the transducer face. A larger angle (due to a steeper trajectory), renders the needle less conspicuous. The angle effect can be managed in most cases by planning a procedure for a shallower trajectory or using a heel-toe maneuver (discussed subsequently in this document) to bring the transducer face into a more parallel arrangement with the needle. An oblique standoff maneuver may also be used to increase needle-transducer colinearity and therefore needle conspicuity and may be particularly useful in superficial regions with little subcutaneous tissue. The ultrasound screen depicts an echogenic dot (Figure 2B), which may represent either the shaft or tip, depending on the relationship between the transducer and the needle. In clinical settings, the clinician would keep the transducer over the needle tip using the techniques described in the text (eg, "walk-down" maneuver). Correlative ultrasound image demonstrating the 10 appearance of the needle with the transducer-needle arrangement shown in Figure 2A. The ultrasound beam cuts a cross section of the needle, producing an echogenic dot on the screen. The challenge is that, based on this single still image, the clinician cannot tell whether this echogenic dot represents the shaft or the needle tip. Thus, the clinician will advance the needle only to the point at which the echogenic dot first appears on the screen, which represents the initial passage of the needle tip under the transducer. Due to the tendency of the needle to pass beyond the transducer using the out-of-plane approach, confirmatory orthogonal in-plane imaging (Figure 1) should be obtained when possible. The needle is advanced perpendicular to the long axis of the transducer such that only the needle tip is visualized. Typically, the target is centered on the ultrasound screen, and the needle is passed under the transducer halfway between the left and right ends. The tip of the needle manifests as a hyperechoic "dot" in the center of the screen. As soon as the "dot" is visualized, the clinician stops advancing the needle to keep the tip within the plane of the beam. A common error among less experienced clinicians is to pass the tip beyond the transducer. The first needle pass is typically shallow, and the needle is successively partially withdrawn, angled more steeply, and then advanced toward the target depth: the so-called walk-down maneuver. Some manufacturers have placed a mark halfway across the long axis side of the transducer to facilitate accurate placement of the needle in the center of the transducer for the out-of-plane approach. The out-of-plane approach is typically used for superficial injections with minimal surrounding soft tissues and is also popular for intravascular needle or catheter placement. It has traditionally been performed using a freehand technique, although applicable needle guides are available.
