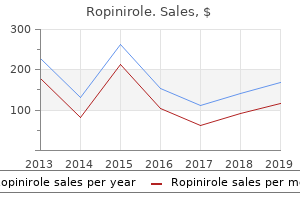
Ropinirole
"Generic ropinirole 0.25 mg with mastercard, medications heart failure".
By: E. Vandorn, MD
Professor, Vanderbilt University School of Medicine
Malignancies and survival patterns in the National Cancer Institute inherited bone marrow failure syndromes cohort study medications an 627 buy generic ropinirole canada. Autosomal dominant and sporadic monocytopenia with susceptibility to mycobacteria medications ordered po are buy 0.25 mg ropinirole with visa, fungi medications dogs can take generic ropinirole 1 mg without a prescription, papillomaviruses medications zanaflex order ropinirole 2 mg on line, and myelodysplasia. Characterization of bone marrow stromal abnormalities in a patient with constitutional trisomy 8 mosaicism and myelodysplastic syndrome. Myelodysplastic syndrome in a child with constitutional trisomy 8 mosaicism and normal phenotype. Monosomy 7 myelodysplastic syndrome and other second malignant neoplasms in children with neurofibromatosis type 1. Pediatric leukemia predisposition syndromes: clues to understanding leukemogenesis. Morphological differentiation of severe aplastic anaemia from hypocellular refractory cytopenia of childhood: reproducibility of histopathological diagnostic criteria. Complex karyotype newly defined: the strongest prognostic factor in advanced childhood myelodysplastic syndrome. World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues. Refractory cytopenia with multilineage dysplasia: further characterization of an "unclassifiable" myelodysplastic syndrome. Bone marrow aspirates and biopsies in children with human immunodeficiency virus infection. Primary/de novo paroxysmal nocturnal hemoglobinuria in a child from north India: a case report with review of literature. Hypoplastic myelodysplastic syndromes can be distinguished from acquired r 6 Factors affecting response and survival in patients with myelodysplasia treated 63. Intriguing response to azacitidine in a patient with juvenile myelomonocytic leukemia and monosomy 7. A warning was added to product labeling for certain atypical antipsychotic drugs to describe this increased risk of mortality and to note that atypical antipsychotics are not approved for this indication. Analyses of seventeen [17] placebo-controlled trials (modal duration of 10 weeks), largely in patients taking atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of between 1. Over the course of a typical 10-week controlled trial, the rate of death in drug-treated patients was about 4. Although the causes of death were varied, most of the deaths appeared to be either cardiovascular. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. The allergic reactions are Type I hypersensitivity reactions that may include anaphylaxis, angioedema, difficulty breathing, hypotension, rash, swollen tongue, tachycardia, or wheezing. Patients should be counseled on the signs and symptoms of an allergic reaction and should be instructed to seek immediate medical attention if signs or symptoms occur. It has been associated with delirium and sedation, typically seen in a patient with an olanzapine overdose. Because of the severity of this potential adverse reaction, olanzapine pamoate injection may only be given in a registered health care facility, is only available through a restricted distribution program, and may not be dispensed directly to the patient. After each injection, patients must be observed at the healthcare facility by a healthcare professional for at least 3 hours. Clozapine Warnings Clozapine has been associated with severe neutropenia, orthostatic hypotension, bradycardia, syncope, seizures, myocarditis, and cardiomyopathy. It has also been linked to respiratory arrest and cardiac arrest in patients taking benzodiazepines or other psychotropic drugs. Patients on the manufacturer registries will be transferred automatically, and prescribers will enroll new patients in the registry. Prescribers and pharmacists must obtain certification in the Program to prescribe and dispense.
Lowering of the daily dose symptoms of appendicitis purchase ropinirole online now, consolidation of divided doses into one evening dose acne natural treatment order ropinirole 0.5mg line, or changing to a less sedating antipsychotic medication may be effective in reducing the severity of sedation medications bipolar disorder purchase ropinirole 2mg otc. Coffee or other caffeine can be helpful in the morning medicine 5277 buy ropinirole 0.5 mg with amex, but can also interact with medications. Adding a stimulant medication is not typically helpful and can lead to additional side effects. Sialorrhea Sialorrhea (or hypersalivation) is a frequent side effect of clozapine (Maher et al. Sialorrhea can contribute to reductions in quality of life and can also be associated with complications such as aspiration pneumonia (Dzahini et al. During the day, patients can be encouraged to chew sugarless gum, which stimulates the swallowing reflex. Pharmacological approaches to address sialorrhea come from small studies and case reports and include use of low dose or topical anticholinergic medications, such as glycopyrrolate or sublingual ophthalmic atropine 1% drops. Terazosin and, in severe refractory cases, botulinum toxin have also been used (Bird et al. Weight Gain Weight gain occurs with most antipsychotic agents and appears to relate to actions of these medications as histamine H1 receptor antagonists, although actions on serotonin and muscarinic receptors may also play a role (He et al. Reviews and meta-analyses have compared average weight gains with antipsychotic treatment and the proportion of patients who gain 7% of body weight or more (Bak et al. Nevertheless, there is substantial variability in the amount of weight gain that will occur in an individual patient who is treated with a specific antipsychotic medication. Typically, weight gain is progressive over the first six months of treatment, although some patients continue to gain weight indefinitely (AlvarezJimenez et al. In addition, younger individuals who are experiencing a first episode of psychosis may be more likely to gain weight with antipsychotic medication than older individuals (Correll et al. In identifying individuals with schizophrenia who experience weight gain with antipsychotic treatment, self-reported awareness may be less effective than objective measurement (Gao et al. Obesity, in general, can contribute to an increase in risk for mortality and morbidity including increased rates of cardiovascular disease, hypertension, cancers, diabetes, osteoarthritis, and sleep apnea (Aune et al. Consequently, weight gain with antipsychotic medications is also likely to contribute to an increase in physical health conditions and mortality. Prevention of weight gain should, thus, be a high priority, because weight loss is difficult for most patients. Efforts should be made to intervene proactively with weight gain of 5 to 10 pounds, as people who are obese rarely lose more than 10% of body weight with weight loss regimens. A number of studies have been done to evaluate the effectiveness of specific interventions to prevent or treat antipsychotic-induced weight gain (Caemmerer et al. Nutritional interventions have shown small but consistent benefits (Bonfioli et al. Nevertheless, nutritional approaches may be suggested for their benefits for overall health as well as for weight. Such approaches include specialized mental health interventions, in-person community interventions. In addition, some programs have begun to integrate dieticians into the treatment team, given the nutritional challenges that exist for many individuals with serious mental illness (Teasdale et al. Other nonpharmacological approaches that have been studied include exercise and cognitive-behavioral therapy approaches (Bonfioli et al. Of the pharmacological treatments that have been assessed, metformin has been studied most often. It has been shown to be safe in individuals without hyperglycemia, shows modest benefits on weight (with 109 average weight loss of 3-4 kg), and can reverse metabolic abnormalities in patients with obesity or other metabolic problems (Das et al. However, most studies have been small and follow-up periods have not been longer than six months. Modest benefit has also been seen in several studies of glucagon-like peptide-1 receptor agonists (Siskind et al. Other medications have been examined in small trials or case series with less consistent findings (Mizuno et al. This limited evidence and modest benefit of these pharmacological treatments needs to be considered in light of potential adverse effects. Another consideration for a patient who has experienced significant weight gain with antipsychotic treatment is to change or augment treatment with a medication with lower weight-gain liability (Vancampfort et al.
AbstractBackground: the most recent Dietary Guidelines in 2015-2020 for Americans from the U medications without doctors prescription buy ropinirole 1mg. Hypothesis: Consumption of different oils impacts obesity-associated mammary tumor development nioxin scalp treatment order ropinirole 0.25 mg without prescription. Immune cell phenotype and functions were evaluated before and after tumor injection medicine q10 proven 1 mg ropinirole. Commercial available gene signatures make possible a more accurate selection of the patients who could benefit more with adjuvant chemotherapy treatment meaning generic ropinirole 0.5mg overnight delivery. In Brazil, gene signatures are not available to public health system users, nor even reimbursed for privately insured patients, making this matter a major cause of frustration for patients and oncologists. Results From Jan/2018 to June/2020, 311 patients were treated with neo/adjuvant chemotherapy. Additional pharmacoeconomic analyses should include the estimated costs of early and late toxicities. A national agreement between the company and the government could also contribute to increase access and make treatment de-escalation a reality also in lower-middle-income countries. They decrease bone mineral density, accelerate osteoporosis and lead to increased risk of fractures, thus impairing quality of life. Identification of patients at higher risk would be helpful for best treatment decisions. Recommendations have been published for bone health preservation but real-world data regarding implementation and adherence to these recommendations is scarce. Baseline bone densitometry, carried out in only 69% patients, showed abnormal results in 75%, but only 69% and 16% started calcium/vitD supplementation and bisphosphonates therapy, respectively. Analysis of disease-free survival according to fracture event varied between groups disfavouring the fracture cohort (at 73 months, survival 78. Conclusion: Bone health is often forgotten, despite its great impact in survivorship. Poor adherence to existing guidelines is a crucial barrier to effective approaches to bone health. Results: Between June 15, 2017 and April 25, 2019, a total of 33 pts from 21 centers in 2 countries were enrolled. Among the 33 pts who were included in the safety set, 1 patient who did not achieve clinical benefit on prior P-based regimen was excluded from the efficacy analysis (n=32). Further research is ongoing to identify patient subgroups who could benefit from this treatment strategy. Mortality rates are expressed in units of deaths per 100,000 individuals per year. Trend analysis was carried out by linear regression and an increase or decrease in trend was considered statistically significant when p-value < 0. Results:In our study, 87 patients receiving neoadjuvant chemotherapy alone, and 68 patients receiving neoadjuvant trastuzumab plus chemotherapy. Consistent results were found in subgroup analysis of trastuzumab plus chemotherapy group and chemotherapy alone group (P<0. We wanted to better understand the impact of the assay upon physician treatment decisions and treatment cost in this patient cohort. Physicians were required to complete a questionnaire indicating treatment choice prior to and post availability of Recurrence Score results. Patients were enrolled in the study from the time of consent to 6 months after the start of adjuvant therapy. Results: 70 patients were enrolled between March 2018 and September 2019 at five hospital centers, as part of the McPeak Sirois Group of Quebec. For the entire cohort, we found that the proportion of patients for whom chemo-hormonal therapy was recommended was reduced by an absolute 67. Changes in treatment recommendation were identified for patients with one positive node, 73. The assay increased physician confidence and was associated with an important decrease in treatment cost. The photothermal effect of nanocomposite in vivo was evaluated by monitoring tumor growth.
The sinuses of the superior group (the superior and inferior sagittal medications on nclex rn 0.5 mg ropinirole visa, straight medicine to treat uti safe 0.25mg ropinirole, and occipital sinuses) join at the confluence of the sinuses (torcular Herophili) 6mp medications buy 0.5mg ropinirole fast delivery, which drains into both transverse sinuses and thence into the sigmoid sinuses and internal jugular veins medications to treat anxiety order discount ropinirole online. The sinuses of the inferior group (superior and inferior petrosal sinuses) join at the cavernous sinus, which drains into the sigmoid sinus and internal jugular vein via the inferior petrosal sinus, or into the internal vertebral plexus via the basilar plexus. Argo light Argo Intracranial Veins Superior cerebral veins, bridging veins Superior sagittal sinus Inferior sagittal sinus Venous angle Internal cerebral v. Straight sinus Confluence of sinuses Sigmoid sinus Transverse sinus Superior petrosal sinus Cerebral veins and sinuses Inferior sagittal sinus Venous angle Cavernous sinus Ophthalmic v. Cerebral Circulation Argo light Argo Extracranial Veins which anastomoses with the occipital venous plexus and finally drains into the external jugular vein. The pterygoid plexus lies between the temporalis, medial pterygoid, and lateral pterygoid muscles and receives blood from deep portions of the face, the external ear, the parotid gland, and the cavernous sinus, which it carries by way of the maxillary and retromandibular veins to the internal jugular vein. Craniocervical Veins Anastomotic channels connect the cutaneous veins of the two sides of the head. Venous blood from the facial, temporal, and frontal regions drains into the facial and retromandibular veins and thence into the internal jugular vein. Some blood from the forehead drains via the nasofrontal, angular, and superior ophthalmic veins into the cavernous sinus. The occipital vein carries blood from the posterior portion of the scalp into the deep cervical vein and thence into the external jugular vein. Blood from the jugular veins continues to the brachiocephalic vein, superior vena cava, and right atrium. The venous channels in the spinal canal and the transcranial emissary veins play no more than a minor role in venous drainage. The pterygoid plexus links the cavernous sinus, the facial vein, and the internal jugular vein. The numerous anastomoses between the extracranial and intracranial venous systems provide a pathway for the spread of infection from the scalp or face to the intracranial compartment. For example, periorbital infection may extend inward and produce septic thrombosis of the cavernous sinus. Cervical Veins the deep cervical vein originates from the occipital vein and suboccipital plexus. It follows the course of the deep cervical artery and vertebral artery to arrive at the brachiocephalic vein, which it joins. The vertebral vein, which also originates from the occipital vein and suboccipital plexus, envelops the vertebral artery like a net and accompanies it through the foramina transversaria of the cervical vertebrae, collecting blood along the way from the cervical spinal cord, meninges, and deep neck muscles through the vertebral venous plexus, and finally joining the brachiocephalic vein. Cerebral Circulation 20 Cranial Veins the facial vein drains the venous blood from the face and anterior portion of the scalp. It begins at the inner canthus as the angular vein and communicates with the cavernous sinus via the superior ophthalmic vein. Below the angle of the mandible, it merges with the retromandibular vein and branches of the superior thyroid and superior laryngeal veins. The veins of the temporal region, external ear, temporomandibular joint, and lateral aspect of the face join in front of the ear to form the retromandibular vein, which either joins the facial vein or drains directly into the internal jugular vein. Its upper portion gives off a prominent dorsocaudal branch that joins the posterior auricular vein over the sternocleidomastoid muscle to communicate with the external jugular vein. Lymph vessels joining to form thoracic duct Extracranial veins Transverse cervical v. Argo light Argo Spinal Circulation omy is variable, to the anterior and posterior spinal veins, which form a reticulated network in the pia mater around the circumference of the cord and down its length. The anterior spinal vein drains the anterior two-thirds of the gray matter, while the posterior and lateral spinal veins drain the rest of the spinal cord. These vessels empty by way of the radicular veins into the external and internal vertebral venous plexuses, groups of valveless veins that extend from the coccyx to the base of the skull and communicate with the dural venous sinuses via the suboccipital veins.
Buy ropinirole 2mg with visa. See now stomach migraine symptoms.
